Symptom Patterns
Premenstrual disorders like PMDD and PME are increasingly understood as a sensitivity to hormone fluctuations. Hormone sensitivity can vary from person to person, and your symptoms may be linked to your unique pattern of sensitivity.
Symptom patterns vary from person to person.
Yes. Recent research from members of our Clinical Advisory Board recommends looking at PMDD and PME as a range of symptoms that can vary in severity or change over time. For example, if you experience rage as one of your symptoms, then instead of asking whether or not rage is present every cycle, this approach suggests looking at the intensity of your rage, how severe it felt. Did it feel more intense this cycle because of work stress? Was it less severe because you had more fun activities planned?
This work also highlights that one can be sensitive to any of the following combinations of ovarian hormone fluctuations:
Rise OR fall in estrogen
Rise OR fall in progesterone
This means that one can be sensitive to more than one kind of hormone fluctuation, and the timing of your symptoms may depend on your unique sensitivity profile, because, as we know, ovarian hormones fluctuate based on specific events in the menstrual cycle.
It also gives you an opportunity to consider symptom patterns more broadly. Currently, only PMDD is recognized as a disorder by the DSM-V and ICD-11 classification systems. However, research is showing that not all people fit into this diagnostic criteria. PME is still considered a phenomenon and not a specific diagnosis, which means not many people recognize that you can still show more severe symptoms of an existing condition at different points in the menstrual cycle. Please note that this work needs further research and there could be more patterns to consider than the ones listed below.
This approach suggests the following types of symptom patterns based on changes in mood and emotions.
1. Symptoms starting in the luteal phase
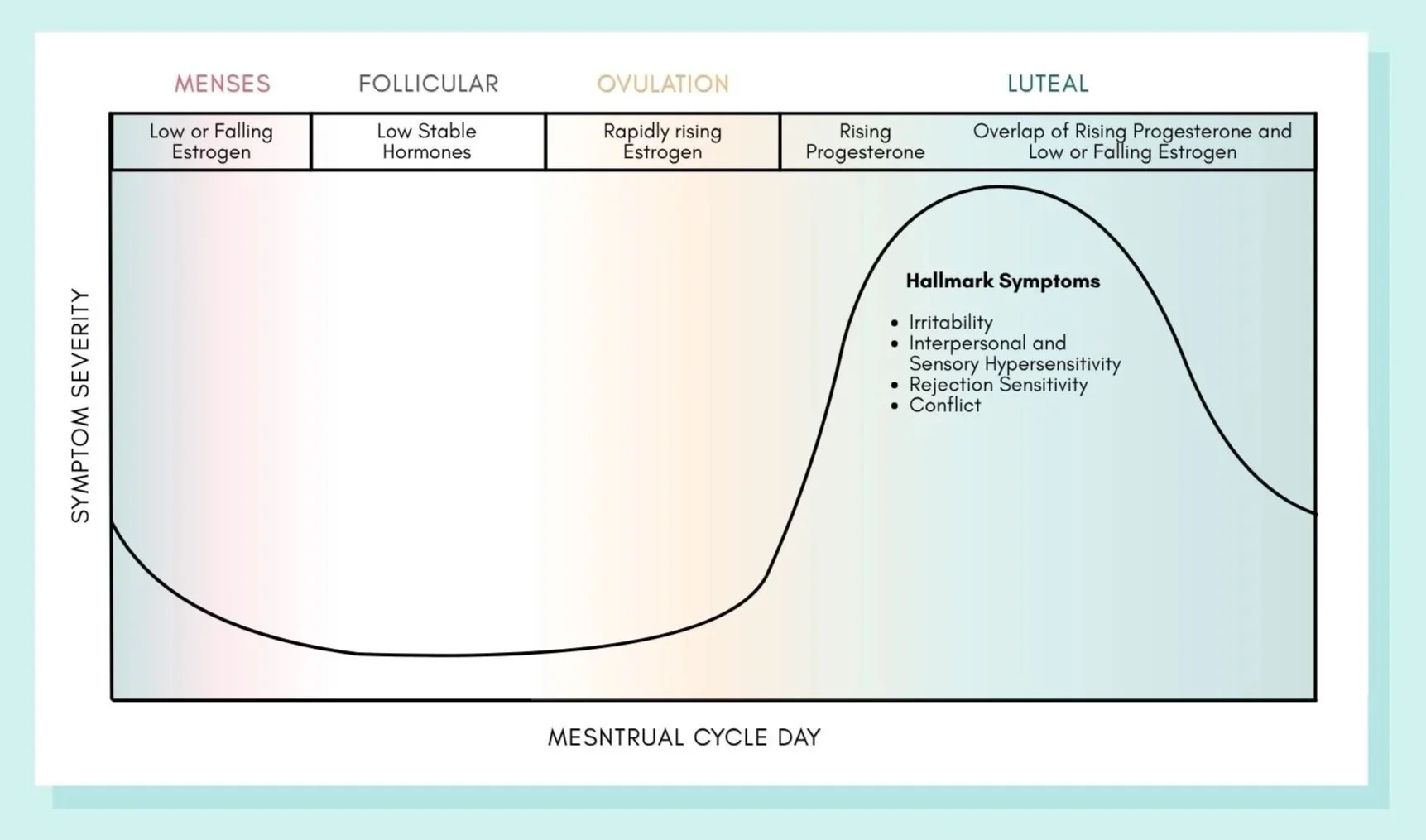
Figure is for illustrative purposes only. Adapted from Peters et al., (2025). DASH-MC Framework published in Molecular Psychiatry.
So far, studies in PMDD typically refer to this type of symptom pattern. It suggests a sensitivity to progesterone and its derivatives, in the luteal phase. The hallmark of this pattern is that your symptoms:
Start after ovulation when there is rising progesterone in your body
Become more severe across the luteal phase (premenstrual week) when progesterone levels peak
Improve within a few days of your period when progesterone levels fall
Go away completely in the follicular phase when progesterone levels are stable and low
Again, this pattern can vary from person to person. Some of you may experience symptoms right after ovulation, or you may experience symptoms only in the week before your period. Nevertheless, these symptoms are considered as “luteal-onset”, meaning they start in the luteal phase and the peak severity of these symptoms are confined to the luteal phase (or premenstrual week).
If this is your pattern, it could mean that you may experience more negative emotions, especially increases in irritability, anger, reduced tolerance for stressful situations, anxiety, mood swings like sudden tearfulness or rage, and a sensitivity to rejection from others. Studies also show that if this is the dominant pattern, then the most bothersome symptoms might include irritability, anger and interpersonal conflict. It may also present as an increased sensitivity to sound alongside increased irritation. This does not mean that you may not experience low mood or hopelessness, but that you are more likely to feel irritated, upset or anxious during your luteal phase and that these symptoms might improve faster once your period starts, compared to someone who experiences more depressive symptoms.
This pattern was also found in PME. For example, studies in borderline personality disorder suggest increased irritability and anger across the luteal phase. In those with a panic disorder, these symptoms may present as increased anxiety during the luteal phase.
2. Symptoms starting around your period
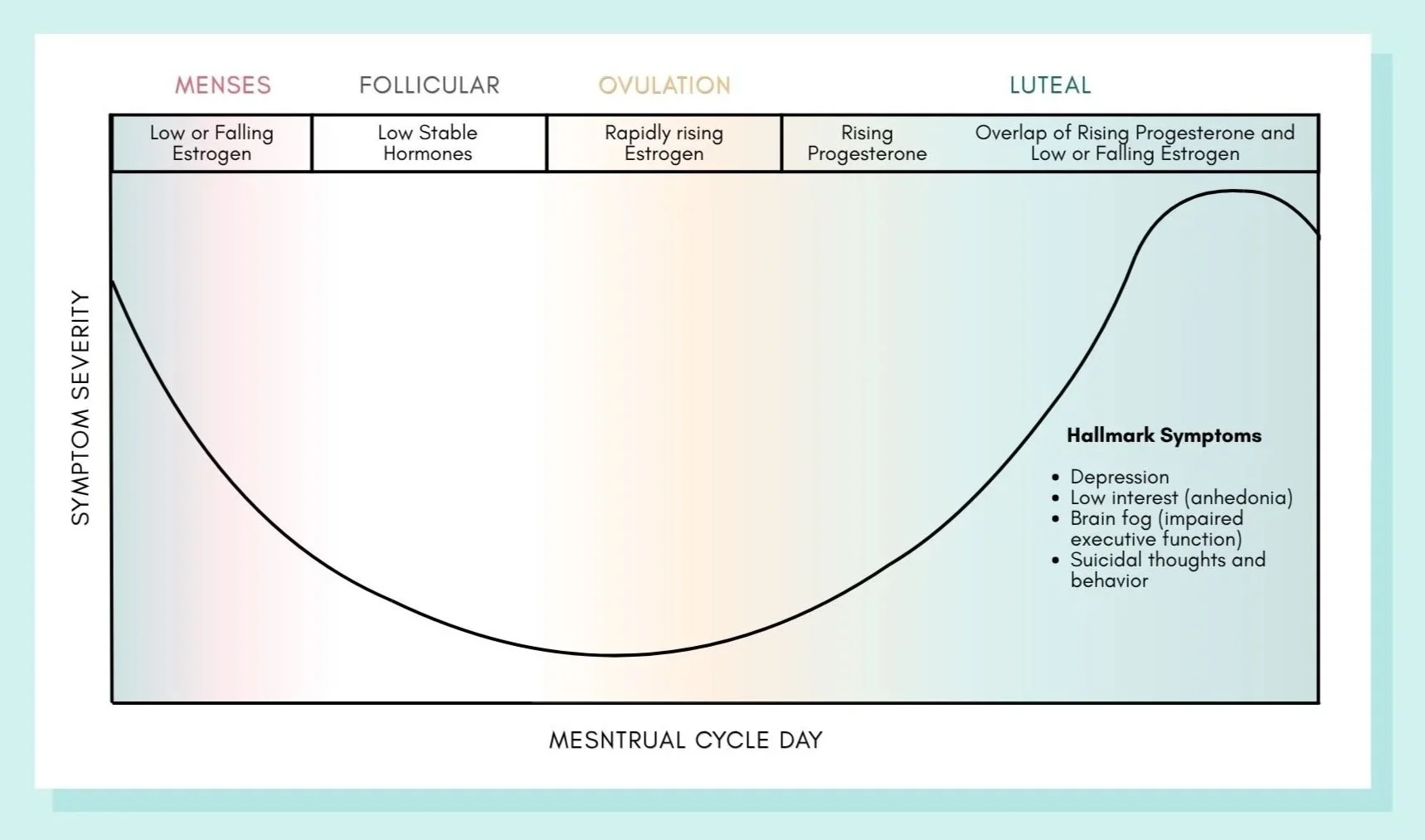
Figure is for illustrative purposes only. Adapted from Peters et al., (2025). DASH-MC Framework published in Molecular Psychiatry.
This second type of symptom pattern is associated with the onset of depressed mood or cognitive symptoms like brain fog around the time of your period (or the perimenstrual phase). It suggests sensitivity to low or declining estrogen levels during the menstrual cycle. The hallmark of this pattern is that your symptoms:
Start closer to your period when estrogen levels plummet
May persist even after your period and extend into your follicular phase as estrogen remains low
Go away completely, only later in the follicular phase when estrogen levels start rising again
In this symptom pattern, your predominant symptoms might include depressed mood, overwhelm, hopelessness, suicidal thoughts or behaviours and difficulties with attention, memory or learning (brain fog). This type of symptom pattern is found in at least two-thirds of people with PMDD, while most patients may also report irritation throughout their luteal phase. In PME, those with borderline personality disorder may experience a worsening of hopelessness, shame and sadness closer to their period (late luteal phase), and it may extend into their follicular phase.
Research also shows that suicide risk increases around one’s period, in line with falling estrogen and progesterone levels. Among those who went to the ER or were hospitalized, suicide attempts were most common around their period. Research also suggests that severity of suicidal thoughts were more common during one’s period than their late luteal phase (premenstrual week) and could extend into their follicular phase (a few days after their period).
3. Symptoms starting around ovulation
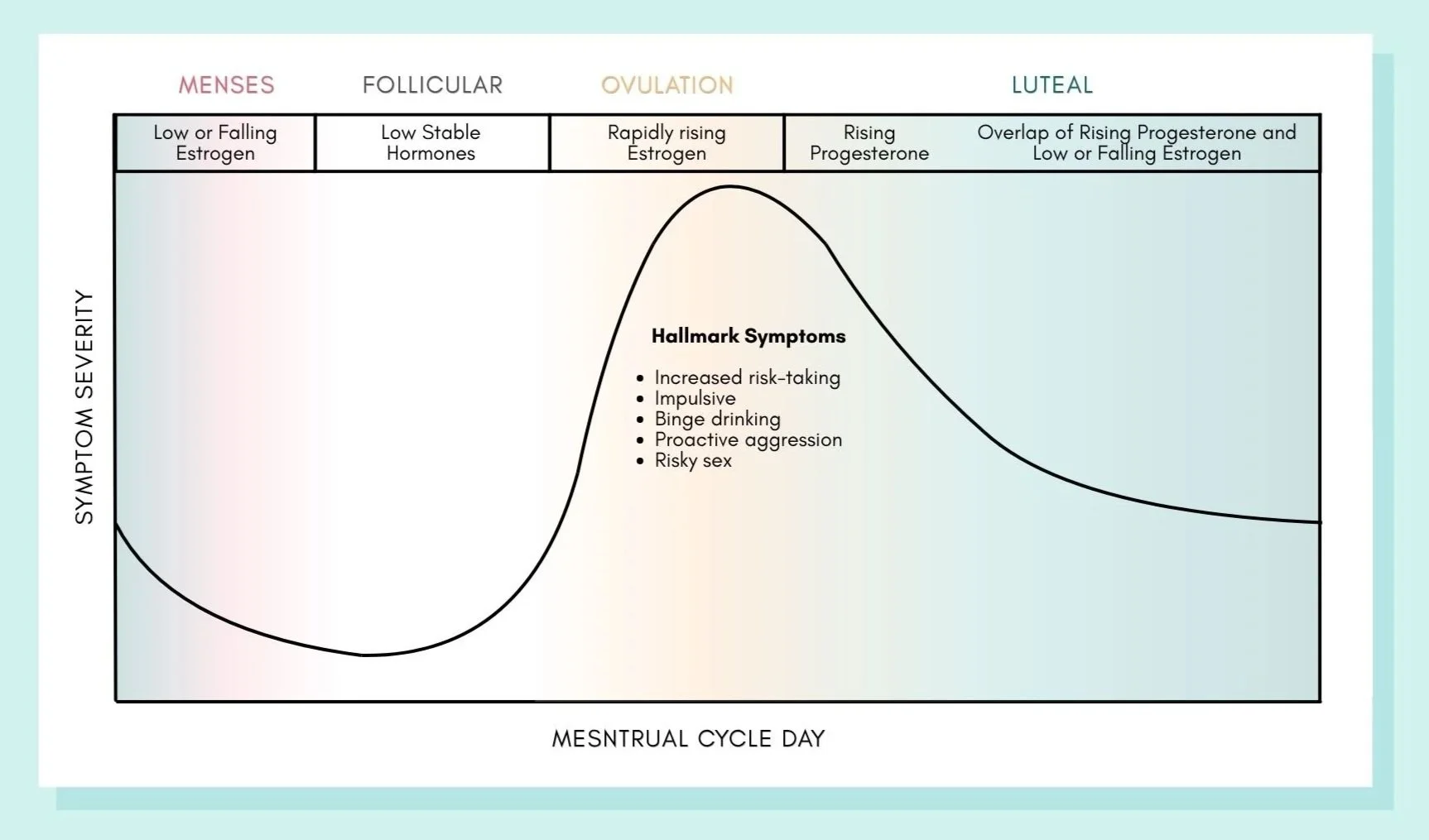
Figure is for illustrative purposes only. Adapted from Peters et al., (2025). DASH-MC Framework published in Molecular Psychiatry.
There is very little research on this symptom pattern, but it suggests that some people may be sensitive to rising estrogen around ovulation. The hallmark of this pattern is that your symptoms:
Start closer to ovulation when there is an acute rise in estrogen
May feel different from your symptoms in the luteal or perimenstrual phase
May feel more impulsive and less emotionally driven
Typically, in those who are hormone-sensitive, the time around ovulation feels less emotional and more driven, with better planning or organizational skills. However, in some people, it can also increase substance use, like increased social drinking or binge drinking, and risky behaviors like increased gambling.
In borderline personality disorder, it could mean an increase in aggression, with the intention to meet their needs (as opposed to reacting aggressively as an emotional response). For example, you might lash out verbally or make dramatic statements, not because you are inherently angry, but because it’s an attempt to achieve a specific goal, like seeking validation or preventing yourself from feeling rejected.
In those with bipolar disorder, case reports suggest a worsening of mania around ovulation. For example, you might start new projects, spend more money than you typically would, and talk rapidly with lots of ideas. Your energy may become extremely intense, making it difficult for you to sit still or sleep.
If you relate to some of these examples but haven’t been diagnosed with borderline personality disorder or bipolar disorder, it doesn’t necessarily mean you have these conditions. Rather, these examples highlight how intense emotional reactions or impulsive behaviors can occur, but may be more pronounced or persistent in certain mental health conditions. It’s a reminder that seeking clarity from a professional can be helpful in understanding what’s typical versus what may require support.
How can recognizing my symptom patterns help?
As mentioned earlier, symptom patterns are unique to you and your experiences. Understanding your unique symptom pattern can help clarify which symptoms bother you the most and when they are likely to show up.
For example, you may experience anger and irritability for almost the entire luteal phase (i.e., two weeks before your period), and it subsides when your period starts. Or, you may experience anger and irritability for the most part, but also feel sad, hopeless, or overwhelmed closer to your period. Your symptoms may change as you approach your period.
Understanding your symptom patterns can help you choose strategies that can help you to cope in the moment. While you may not always be able to change your thoughts when you’re feeling intense rage, you can try engaging your senses, such as dunking your face in cold water or doing an intense workout, to reduce the intensity. On the other hand, if you’re feeling sadness or hopelessness, you can consider shifting your focus to activities that bring you joy or a sense of accomplishment. Maybe that’s taking a relaxing bath or baking your favorite pie. By recognizing your symptoms, you can empower yourself to discover what works best for you.
-
Baca-Garcia, E., Diaz-Sastre, C., Ceverino, A., Perez-Rodriguez, M. M., Navarro-Jimenez, R., Lopez-Castroman, J., et al. (2010). Suicide attempts among women during low estradiol/low progesterone states. Journal of Psychiatric Research. 44, 209–214. https://doi.org/10.1016/j.jpsychires.2009.08.004
Barone, J. C., Ross, J. M., Nagpal, A., Guzman, G., Berenz, E., Pang, R. D., et al. (2023). Alcohol use and motives for drinking across the menstrual cycle in a psychiatric outpatient sample. Alcoholism: Clinical and Experimental Research. 47, 127–142. https://doi.org/10.1111/acer.14971
Eisenlohr-Moul, T. A., Kaiser, G., Weise, C., Schmalenberger, K. M., Kiesner, J., Ditzen, B., et al. (2020). Are there temporal subtypes of premenstrual dysphoric disorder? Using group-based trajectory modeling to identify individual differences in symptom change. Psychological Medicine. 50, 964–972. https://doi.org/10.1017/S0033291719000849
Eisenlohr-Moul, T. A., Schmalenberger, K. M., Owens, S. A., Peters, J. R., Dawson, D. N., & Girdler, S. S. (2018). Perimenstrual exacerbation of symptoms in borderline personality disorder: Evidence from multilevel models and the Carolina Premenstrual Assessment Scoring System. Psychological Medicine. 48, 2085–2095. https://doi.org/10.1017/S0033291718001253
Epperson, C. N., Pittman, B., Czarkowski, K. A., Stiklus, S., Krystal, J. H., & Grillon, C. (2007). Luteal phase accentuation of acoustic startle response in women with premenstrual dysphoric disorder. Neuropsychopharmacology. 32, 2190–2198. https://doi.org/10.1038/sj.npp.1301351
Gordon, J. L., & Chenji, S. (2025). Self-guided mental health interventions for premenstrual mood symptoms. Current Psychiatry Reports. 27(12), 758–764. https://doi.org/10.1007/s11920-025-01645-1
Kaspi, S. P., Otto, M. W., Pollack, M. H., Eppinger, S., & Rosenbaum, J. F. (1994). Premenstrual exacerbation of symptoms in women with panic disorder. Journal of Anxiety Disorders. 8, 131–138. https://doi.org/10.1016/0887-6185(94)90011-6
Martel, M. M., Eisenlohr-Moul, T., & Roberts, B. (2017). Interactive effects of ovarian steroid hormones on alcohol use and binge drinking across the menstrual cycle. Journal of Abnormal Psychology. 126, 1104–1113. https://doi.org/10.1037/abn0000304
Owens, S. A., Schmalenberger, K. M., Bowers, S., Rubinow, D. R., Prinstein, M. J., Girdler, S. S., et al. (2023). Cyclical exacerbation of suicidal ideation in female outpatients: Prospective evidence from daily ratings in a transdiagnostic sample. Journal of Psychopathology and Clinical Science. 132(6), 704–715. https://doi.org/10.1037/abn0000838
Peters, J. R., Owens, S. A., Schmalenberger, K. M., & Eisenlohr-Moul, T. A. (2020). Differential effects of the menstrual cycle on reactive and proactive aggression in borderline personality disorder. Aggressive Behavior. 46, 151–161. https://doi.org/10.1002/ab.21877
Peters, J. R., Schmalenberger, K. M., Eng, A. G., Stumper, A., Martel, M. M., & Eisenlohr-Moul, T. A. (2025). Dimensional Affective Sensitivity to Hormones across the Menstrual Cycle (DASH-MC): A transdiagnostic framework for ovarian steroid influences on psychopathology. Molecular Psychiatry. 30(1), 251–261. https://doi.org/10.1038/s41380-024-02693-4
Ross, J. M., Barone, J. C., Tauseef, H., Schmalenberger, K. M., Nagpal, A., et al. (2024). Predicting acute changes in suicidal ideation and planning: A longitudinal study of symptom mediators and the role of the menstrual cycle in female psychiatric outpatients with suicidality. American Journal of Psychiatry. 181, 57–67. https://doi.org/10.1176/appi.ajp.20230303
Saunders, K. E. A., & Hawton, K. (2006). Suicidal behaviour and the menstrual cycle. Psychological Medicine. 36, 901–912. https://doi.org/10.1017/S0033291706007392
Teatero, M. L., Mazmanian, D., & Sharma, V. (2014). Effects of the menstrual cycle on bipolar disorder. Bipolar Disorders. 16, 22–36. https://doi.org/10.1111/bdi.12138