Ovarian Hormones and Mood
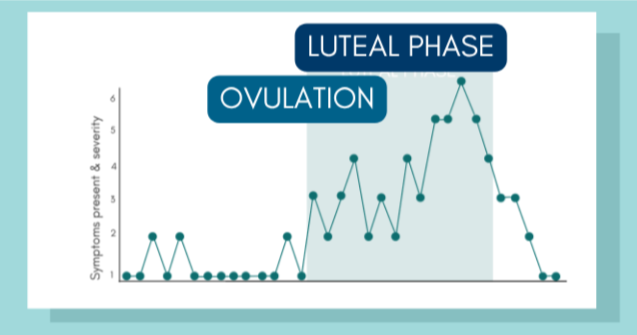
Image is for illustrative purposes only. Adapted from IAPMD’s PMDD Treatment Options ebook.
Premenstrual Dysphoric Disorder (PMDD) was officially considered a diagnosis only recently. It was recognized in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) in 2013 and was included in the International Classification of Diseases (ICD) in 2019.
PMDD is a condition where the week (or two weeks) before a person’s period brings a specific set of emotional, cognitive, and physical changes that are much more intense than typical premenstrual discomfort. These symptoms can interrupt everyday life, relationships, school, or work.
The emotional side often includes things like severe mood swings, deep sadness or hopelessness, intense irritability, anxiety, or feeling on edge. People may suddenly snap at others or feel overwhelmed by emotions that seem disproportionate to the situation. On the cognitive side, it’s common to struggle with concentration, feel drained of energy, lose interest in activities you normally enjoy, or feel like you can’t “cope” the way you usually would. There are also physical symptoms, such as breast tenderness, bloating, headaches, joint or muscle aches, fatigue, and sleep disturbances.
What makes PMDD different from premenstrual moodiness is its severity and timing. The symptoms show up reliably in the luteal phase (the last 2 weeks before your period), and they go away within a few days of when menstruation starts. In PMDD, at least five symptoms must be present during this window, including at least one core emotional symptom (like mood swings, irritability, anxiety, or depressed mood).
Diagnosing PMDD isn’t done with a blood test or scan; instead, it requires careful tracking of symptoms across at least two menstrual cycles. The latest research emphasizes that, without this perspective, daily tracking is considered provisional rather than confirmed.
Many clinicians prefer to assess symptoms during natural, ovulatory cycles. This is because if you’re on hormonal birth control that stops or alters ovulation, it can change how symptoms show up or make them harder to interpret.
Newer research pooling data from more than 50,000 people across multiple continents found that about 1-3% meet the strict criteria for PMDD based on daily symptom tracking across two cycles. That’s roughly about 1-3 in 100 people. A larger group of people may have significant premenstrual symptoms but do not meet full diagnostic standards.
Although the DSM-5 sets the diagnostic threshold at five symptoms, research shows that having four symptoms per cycle can already signal meaningful disruption. Each additional symptom raises the likelihood of real-life difficulties, highlighting how intertwined emotional, cognitive, and physical experiences are in shaping the day-to-day impact of PMDD.
In everyday terms, someone with PMDD isn’t just feeling “cranky” before a period. Their emotional and physical state shifts so dramatically and predictably each month that it’s noticeable to them and often to others, and when it interferes with life, especially work, relationships, and school, it is important to consider seeking medical advice.
-
Barone, J.C., Romano, R., Nagpal, A. et al. Peripheral cyclical expression of GABA-A receptor subunit genes and menstrual cycle affective change: a dimensional, transdiagnostic study. Transl Psychiatry15, 533 (2025). https://doi.org/10.1038/s41398-025-03767-9
Rubinow, D. R., Schmidt, P. J., & Roca, C. A. (1998). Estrogen–serotonin interactions: implications for affective regulation. Biological Psychiatry, 44(9), 839-850. https://doi.org/https://doi.org/10.1016/S0006-3223(98)00162-0